Frequently Asked Questions
- How many RVUs does an average Radiologist read every year?
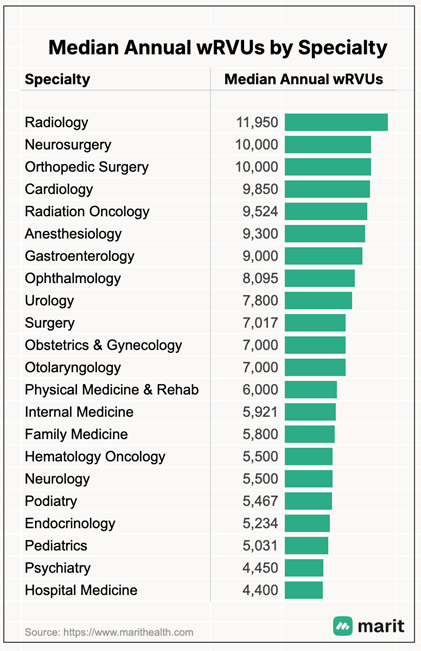 Radiologist annual productivity varies greatly based on 4 major variables: practice type (academic vs private practice), practice location (hospital based, outpatient imaging center, teleradiology), subspeciality (neuroradiology, interventional radiology or pediatrics, for example) and individual speed or motivation. Additional variables include vacation time, shift intensity, and individual group staffing and compensation models. The annual range can be below 8,000 wRVUs for some subspeciality academic radiologists to greater than 14,000 for some subspecialty teleradiologists who don’t have the same teaching and/or administrative responsibilities. Most of the data that is collected nationally regarding annual wRVUs is not published. According to Marit Health, the average for radiologists is 11,950 in 2025.
Radiologist annual productivity varies greatly based on 4 major variables: practice type (academic vs private practice), practice location (hospital based, outpatient imaging center, teleradiology), subspeciality (neuroradiology, interventional radiology or pediatrics, for example) and individual speed or motivation. Additional variables include vacation time, shift intensity, and individual group staffing and compensation models. The annual range can be below 8,000 wRVUs for some subspeciality academic radiologists to greater than 14,000 for some subspecialty teleradiologists who don’t have the same teaching and/or administrative responsibilities. Most of the data that is collected nationally regarding annual wRVUs is not published. According to Marit Health, the average for radiologists is 11,950 in 2025.- How many RVUs does an average radiologist read in a shift?
- This is highly variable based on type of shift, practice type and individual group’s staffing model. A private practice Emergency Radiology shift would be greatly different than an average Academic Chest Radiologist responsible for high volume in-patient chest radiographs, for example, given the relative value of the studies. For a radiologist reading 12,000 wRVUs a year over 200 annual working days is 60 wRVUs per day, versus a radiologist reading 8,000 wRVUs a year over 200 clinical days is 40 RVUs a day.
- What are the average billable charges for an average radiologist annually?
- A radiologist reading 12,000 wRVUs annually generates on average over $600,000 in physician charges as well as over 2.5M in practice expense charges (technical charges).
- Which radiology subspecialties generate the most or the least RVUs?
- While annual wRVUs has many variables, some subspecialties in radiology average higher annual wRVU numbers because of a favorable mix of cases. Emergency and Neuroradiologists tend to be on the higher end with a favorable mix of CT and MRI, but conditions can vary greatly among groups. Nuclear Medicine and Pediatrics tend to be on the lower end. Breast Imaging, Thoracic and Musculoskeletal Radiology tend to be in the middle range. Interventional Radiology is highly variable based on the practice type.
- Why do radiologist salaries vary so much based on location?
- Variation in Radiologist salaries is multifactorial. Beyond pure supply and demand regionally and cost of living, certain geographic locations will have different payor mix, meaning a different percent of Medicare/Medicaid patients compared to patients with private insurance with traditionally have much better reimbursement rates.
- How much does an average radiologist make annually?
 Radiology compensation is a complicated mix of base pay, bonus and benefits which varies by geographic location, type of practice (academic, employed, partner, remote, locums, etc.) and subspecialty.
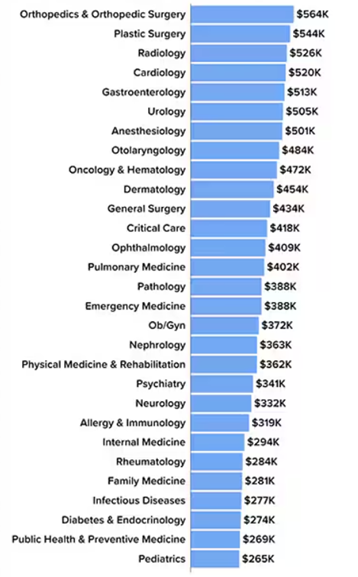
The 2025 Medscape Physician Compensation Report (link) lists Radiology as the 3rd highest earning physician at $526,000 annually for full-time radiologists, based on a total compensation survey.
The AAMC publishes an academic Faculty Salary Report, which is available for purchase and is for personal use only (link).
There are multiple additional consulting firms and private entities that collect physician compensation data and some like Physician Side Gigs (link) publish summaries online which can be helpful to individuals searching for a job or evaluating their current position.
(Jon McKenna July 8, 2025: https://www.medscape.com/slideshow/2025-compensation-overview-6018103)
Radiology compensation is a complicated mix of base pay, bonus and benefits which varies by geographic location, type of practice (academic, employed, partner, remote, locums, etc.) and subspecialty.
The 2025 Medscape Physician Compensation Report (link) lists Radiology as the 3rd highest earning physician at $526,000 annually for full-time radiologists, based on a total compensation survey.
The AAMC publishes an academic Faculty Salary Report, which is available for purchase and is for personal use only (link).
There are multiple additional consulting firms and private entities that collect physician compensation data and some like Physician Side Gigs (link) publish summaries online which can be helpful to individuals searching for a job or evaluating their current position.
(Jon McKenna July 8, 2025: https://www.medscape.com/slideshow/2025-compensation-overview-6018103)
- Why do private practice radiologists often make more than academic radiologists?
- Academic Radiologists traditionally have roles and responsibilities outside of their clinical work which is not reimbursed the same way as reading a CT scan, for example. Teaching Medical Students, training residents and fellows, participating in multidisciplinary conferences (tumor boards), publishing research and other scholarly activity does not generate direct income for a radiologist or group, unless agreements are made between the Health System or School of Medicine. Private Practice Radiologists tend to focus on the billable clinical work. Groups can be organized in different ways to prioritize administrative and non-RVU generating work, or they may abandon the wRVU system entirely. Groups that rely solely on wRVU generation run the risk of devaluing non-RVU generating work necessary to run a successful group.
Glossary: Radiology RVU & Billing Terms
A-C
- ACR (American College of Radiology)
- A professional organization that provides clinical guidelines, accreditation, and advocacy for radiology practices.
- Allowance
- The maximum amount a payor will reimburse for a specific procedure or service.
- Authorization
- Pre-approval from a payor required before performing certain radiology exams (especially MRIs, CTs, and nuclear medicine).
- Bundled Services
- When multiple procedures are combined under one reimbursement, often at a lower rate than if billed separately.
- CPT (Current Procedural Terminology)
- A set of codes developed by the AMA used to describe diagnostic and therapeutic procedures, including radiology exams.
- CMS (Centers for Medicare & Medicaid Services)
- The federal agency that oversees Medicare/Medicaid and sets the RVU values used in physician fee schedules.
- Coding
- The process of translating a radiology service into billing codes (e.g., CPT, ICD-10) for reimbursement.
D–F
- Deductible
- The portion of the bill a patient must pay before their insurance plan covers costs.
- Downcoding
- A claim submitted with a lower-level CPT code than appropriate, often resulting in lost reimbursement.
- Explanation of Benefits (EOB)
- A statement from a payor explaining what was billed, what was covered, and what the patient owes.
- Facility Fee
- A charge billed by the imaging center or hospital for the use of space and equipment, separate from the radiologist’s fee.
G–I
- Geographic Practice Cost Index (GPCI)
- Attempt to adjust for cost of living, practice costs, variations in malpractice cost and wages by location.
- Global Fee
- A single payment covering both the technical and professional components of a radiology service.
- Global Period
- The time during which all services related to a procedure (e.g., post-op imaging for interventional radiology) are considered included in the payment.
- HCPCS (Healthcare Common Procedure Coding System)
- A set of standardized codes used alongside CPT codes, especially for Medicare billing.
- IMG (Independent Medical Group)
- A physician-owned practice or entity that provides professional radiology services independent of a hospital or health system.
- Interventional Radiology (IR)
- A radiology subspecialty that performs image-guided procedures. Often involves more complex billing due to E/M services, sedation, and device use.
M–P
- MAC (Medicare Administrative Contractor)
- A private company contracted by CMS to process Medicare claims, set local coverage policies, and audit radiology billing.
- Modifier
- A two-character code appended to a CPT code to provide additional billing context (e.g., -26 for professional component, -TC for technical component).
- MPFS (Medicare Physician Fee Schedule)
- CMS’s list of fees assigned to CPT codes based on RVUs and other factors.
- MRI (Magnetic Resonance Imaging)
- A common radiology procedure with specific CPT codes that often require prior authorization.
- NCCI Edits (National Correct Coding Initiative)
- CMS rules that determine which procedures can or cannot be billed together.
- Payor Mix
- The percentage breakdown of a practice’s revenue by insurance type (e.g., Medicare, Medicaid, commercial, self-pay). Influences overall reimbursement rates and financial planning.
P–R
- Precertification / Prior Authorization
- Approval from a payor required before specific imaging exams are performed; denial may lead to non-payment.
- Professional Component (PC)
- The portion of a radiology service provided by the interpreting physician (e.g., reviewing images, writing the report).
- Practice Expense RVU
- The component of an RVU reflecting costs of non-physician resources (equipment, techs, supplies).
- RBRVS (Resource-Based Relative Value Scale)
- A system used by Medicare to determine physician payment based on work RVU, practice expense, and malpractice RVU.
- Revenue Cycle Management (RCM)
- The full process of billing, coding, collections, and claim follow-up from patient registration to payment.
- RVU (Relative Value Unit)
- A unit measuring the value of medical services for reimbursement. Composed of work RVUs, practice expense, and malpractice components.
S–Z
- Self-Pay
- When a patient pays directly for services without insurance. Typically involves discounted or prompt-pay rates.
- Split Billing
- Separating the global fee into professional and technical components, often necessary when billing across different entities.
- Teleradiology
- Remote interpretation of imaging studies. Billing varies depending on licensure, location, and global vs. component-based arrangements.
- Technical Component (TC)
- The portion of a radiology service covering equipment, image acquisition, and staff support.
- Unbundling
- Incorrectly billing separate procedures that should be grouped under a single bundled code. This can trigger audits.
- wRVU (Work Relative Value Unit)
- Reflects the time, skill, training, and intensity required by the physician to perform a procedure. A key component of physician compensation models.